
Steven G. Ayre, Donato Perez Garcia y Bellon and Donato Perez Garcia, Jr. — European Journal of Cancer 1990; 26(11-12):1262-3
We have developed a neoadjuvant chemohormonal therapy for breast carcinomas without surgery or radiotherapy. Cyclophosphamide, methotrexate, and 5-fluorouracil are administered, with insulin as a biological response modifier to potentiate anticancer drug effects [1]. This regimen affords maximum breast conservation and minimum patient discomfort.
Breast malignancies are histologically verified by fine needle biopsy. Insulin/chemotherapy cycles are repeated twice a week for 3 weeks, and then weekly for another 3—6 weeks depending on clinical findings. Fasting subjects receive insulin (0.3 U/kg) and, at onset of hypoglycaemia, cyclophosphamide 8 mg/rn2, methotrexate 3 mg/rn2, and 5-fluorouracil 50 mg/rn2 with 50% hypertonic glucose, intravenously. On non-treatment days, patients are given oral cyclophosphamide 50 mg and methotrexate 2.5 mg.
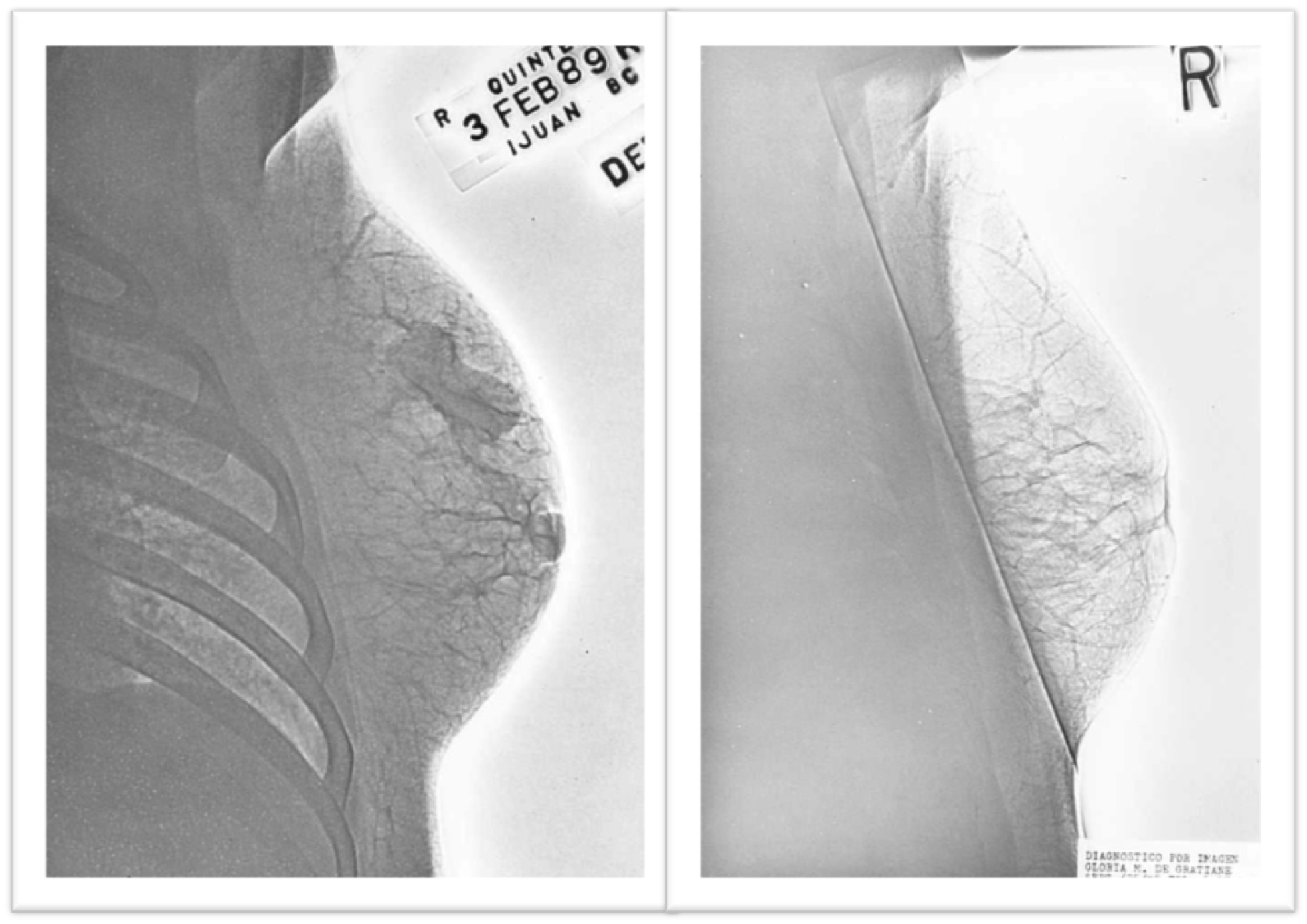
A 32-year-old woman found a lump in her right breast in November 1988. Xeromammography confirmed the presence of a lesion (Fig. 1), and a biopsy revealed an infiltrating ductal adenocarcinoma. After 8 weeks of chemohormonal therapy, the breast mass was no longer palpable. A xeromammogram at 3 months showed no evidence of tumour (Fig. 1).
Insulin and insulin-like growth factor-1 (IGF-1) have been identified as autocrine and/or paracrine growth factors in human breast cancer cells [2-4]. We administer pharmacological doses of insulin to manipulate membrane and metabolic activities of these endogenous growth-promoting mechanisms, thereby potentiating anticancer drug effects. Drug potentiation results from an insulin-induced increase in the transmembrane passage of anticancer drugs in human breast cancer cells [5, 6], and a recruitment of cell populations into S-phase of the replicative cycle by cross-reaction of insulin with IGF-1 receptors [7]. The cell-killing effects of anticancer drugs, particularly the chemotherapy agents specific for cell cycle phase, are greatly augmented [8]. Therefore, ideal pharmacokinetic circumstances for the chemotherapy of breast cancer are created. As well as improved efficacy, this regimen increases safety because of lower total doses administered and reduced side-effects.
Chemohormonal therapy with oestrogen has shown promising results in preliminary trials [9]. However, insulin and chemotherapy is more efficacious, as not only can insulin mimic oestrogen’s cell-recruiting effects in oestrogen receptor positive human breast cancer cells [10], but insulin also stimulates recruitment in oestrogen receptor negative cells. Unlike oestrogen, insulin can increase the transmembrane passage and intracellular accumulation of anticancer drugs. The administration of low-dose anticancer drug therapy with insulin can produce complete and long-term regression of tumour masses in treated subjects. Therapy is tolerated without adverse effect and in our case produced excellent cosmetic results. Fig. 1. Patient 1: xeromammogram on 3 February (left) and 15 June (right) 1989.
1. Ayre SG, Perez Garcia y Bellon D, Perez Garcia D Jr. Insulin potentiation therapy: a new concept in the management of chronic degenerative disease. Med Hypotheses 1986,20, 199-210.
2. Hilf R. The actions of insulin as a hormonal factor in breast cancer. In: Pike MC, Siiteri PK, Welsch CW, eds. Hormones and Breast Cancer. Cold Spring Harbor, Cold Spring Harbor Laboratory, 1981, 317-337.
3. Lippman ME, Dickson RB, Kasid A, et al. Autocrine and paracrine growth regulation of human breast cancer. J Steroid Biochem 1986, 24, 147-154.
4. Cullen JK, Yee D, Sly WS, et al. Insulin-like growth factor receptor expression and function in human breast cancer. Cancer Res 1990, 50,48-53.
5. Alabaster 0, Vonderhaar BK, Shafie SM. Metabolic modification by insulin enhances methotrexate cytotoxicity in MCF-7 human breast cancer cells. Eur J Cancer Clin Oncol 1981, 17, 1223-1228.
6. Oster JB, Creasey WA. Enhancement of cellular uptake of ellipticine by insulin preincubation. Eur 3 Cancer Clin Oncol 1981, 17, 1097-1103.
7. Van Wyk JJ, Graves DC, Casella SJ, Jacobs S. Evidence from monoclonal antibody studies that insulin stimulates deoxyribonucleic acid synthesis through the type 1 somatomedin receptor. 3 Clin Endocrinol Metab 1985, 61,639-643.
8. Shackney SE, Cell kinetics and cancer chemotherapy. In: Calabresi
P, Schein PS, Rosenberg SA, eds. Medical Oncology: Basic Principles and Clinical Management of Cancer, New York, Macmillan, 1985, 41-60.
9. Paridaens R, Klijn JGM, Julien JP, et al. Chemotherapy with estrogenic recruitment in breast cancer: experimental background and clinical studies conducted by the EORTC breast cancer cooperative group. Eur J Cancer Clin Oncol 1986,22,728.
10. Van der Burg B, de Laat SW, van Zoelen EJJ. Mitogenic stimulation of human breast cancer cells in a growth-factor defined medium: synergistic action of insulin and estrogens. In: Brescani F, King RJB, Lippman ME, Raynaud JP, eds. Progress in Cancer Research and Therapy, vol. 35: Hormones and Cancer 3. New York, Raven Press, 1988,231-233.